 The view from the White House.
The view from the White House.
As regular readers of Addiction Inbox will know, I am on record as favoring some form of decriminalization for marijuana. But I also write regularly about the difficulties of marijuana addiction and withdrawal. And I have been critical of the operational strategies employed by the medical marijuana movement in the several states in which it now operates. What I have not done, to date, is offer up the official view of a drug policy analyst from the Obama administration who straightforwardly favors a continuation of the legal prohibition against marijuana.
One of the architects of the current federal resistance to marijuana legalization is
Kevin Sabet, an assistant professor and the director of the Drug Policy Institute at the University of Florida College of Medicine. Sabet served from 2009 to 2011 in the Obama Administration as Senior Advisor for the White House Office of National Drug Control Policy (ONDCP) under Drug Czar Gil Kerlikowske, and was influential in shaping federal marijuana policy. Sabet consults with governments and NGOs on a wide range of drug policy prevention issues, and
recently debated legalization advocate Ethan Nadelmann on CNN. He is also a regular columnist for
thefix.com and
Huffington Post. He agreed to participate in a frank and lengthy 5-question interview with Addiction Inbox.
(Be sure to check out the comments below).
1. In his new book, Too High to Fail, journalist Doug Fine argues that "the Drug War is as unconscionably wrong for America as segregation or DDT." Would you comment on this sweeping condemnation?
First, I think it is interesting to note that only people who want to condemn all of our current drug policies use the term "drug war." No one in serious policy circles uses that term anymore, and that is because it is woefully inadequate and vague as a way to describe a whole slew of policies designed to both reduce drug prevalence and drug consequences. I think his comparison is clumsy and unfair. Do some drug policies hurt disadvantaged groups? Of course they do. Is it a moral imperative to fix those policies, learn from our past mistakes and make our policies better? Of course it is. There's no reason to think that those policies can't be changed—in the White House in 2009, for example, we drastically reduced the penalty for crack cocaine. But what makes Mr. Fine's comparison even more wrong-headed and backwards is that we know that if we scale-up—not eliminate, as he would—the policies we know do work in reducing drug use and its consequences, all communities in America would benefit. A handful include:
(a) community-based prevention that not only focuses on stopping drug use among school kids, but in changing bad local laws and ordinances that promote underage drinking, smoking, and marijuana use (so-called "environmental policies");
(b) early intervention and detection of drug use in health settings;
(c) evidence-based treatment, including methadone and buprenorphine, as well as 12-step programs;
(d) recovery-based policies that don't penalize people for past drug use and instead facilitate recovery;
(e) law enforcement based on credible threats and modest sanctions.
2. The Drug War is an industry—the DEA alone has a budget of 2 1/2 billion and employs almost 10,000 people. If we add in profits from the private prison industry, and the money-laundering banks, the money is staggering. Wouldn't it make sense to recoup those historical costs by legalizing and taxing marijuana?
That phrase assumes two things: (a) criminal justice and regulation costs would be drastically reduced, or eliminated, with marijuana legalization; and (b) the underground market would be eliminated with marijuana legalization. Both of those assumptions are huge leaps that don't stand up to our experience with our already two legal drugs—alcohol and tobacco.
First, we know that legalization means more consumption. More consumption means more regulation. Today we have liquor laws, laws against drinking and driving, laws against public drunkenness, etc. With regards to legal alcohol, we make 2.6 million arrests every year for the violation of those laws. Meanwhile, we arrest a million fewer times for illegal drugs (1.6 million/year). Legal alcohol costs us money with regards to crime and regulation. I think that is a big consideration in this whole debate that we rarely hear about. So that means we'd have to have more prisons, more police, and more regulation costs under legalization—especially since few people are in prison or jail solely for marijuana use.
And I'm not so sure the underground market would be eliminated with marijuana legalization. Especially if it is taxed heavily, the incentive for the underground market—having been painstakingly established for decades by multinational corporate structures (cartels)—is very little. We'll still need a black market for underage marijuana, for marijuana to be sold to repeat offenders, etc. I just don't see the cartels throwing up their hands and saying "OK, it's legalized. We're out of the game now. Let's get into the ice cream business."
3. A "Pax Cannabis" would require rescheduling marijuana at the federal level, with an overt recognition that marijuana has some redeeming medical value. What's the argument for maintaining cannabis as a Schedule 1 drug along with heroin, a drug with which it has almost nothing in common? Could you comment on the upcoming U.S. Appeals Court consideration of medical marijuana?
Rescheduling marijuana is one of the biggest red herrings I can think of in this debate. If rescheduled tomorrow, it would do nothing to allow marijuana to be sold legally. Rather, it would be a huge symbolic victory for marijuana advocates -- but it would be wholly wrong on the science. Placing a drug in schedule 1 simply means the drug has no medical use and a high potential for abuse. It has nothing to do with the other drugs in that category (e.g. heroin). If it were a drug, a telephone would also need to be in Schedule 1 - I'm addicted to my cell phone and I know it has no medical use. That doesn't mean a phone is as dangerous as a syringe of heroin. Today, cocaine is Schedule 2 because it has some very limited hospital use. Can a 21-year-old kid with no medical knowledge sell cocaine from a "dispensary" called "Happy Clinic" legally? Of course not, though that is what is happening [with marijuana] in California.
In order to be used for medical use, a specific product needs to be approved by FDA. Marijuana's specific product, so far, is Marinol, a Schedule 3 drug which has been approved by FDA and is used by people throughout the world.
Crude, raw marijuana is not a specific product. The best way I can put it is this: We don't smoke opium to get the effects of morphine, so why do we think we need to smoke marijuana to get its potential medical effects? We have non-inhaled medications that are approved and we have others on the way. For a lot more on this, you can check out an article I wrote for
Join Together.
I think the District court opinion will rest on the science and agree with the Department of Health and Human Services that raw, crude marijuana is not medicine.
4. Alaska decriminalized marijuana in 1975, and only recriminalized after lengthy pressure from the Reagan administration. Isn't cultivation of this flowering weed for personal use the most obvious and straightforward solution?
The Reagan Administration could have cared less about Alaska, frankly. Alaska recriminalized because voters there wanted that to happen. They didn't like the effect of decriminalization on their state. That said, I don't think many people are in favor—and I am not—of locking up people smoking small amounts of marijuana. That isn't happening anywhere. One notable exception is New York City where they impose 24-hour detentions for public use and selling as part of their broken windows approach to crime control.
Indeed, in the 1970s, twelve states formally decriminalized marijuana. This meant that persons found to have a small amount of marijuana were not subject to jail time, but rather they would receive a civil penalty, such as a fine. The discussion in the United States is highly complex because even in jurisdictions without a formal decriminalization law, persons are rarely jailed for possessing small amounts of cannabis. A rigorous government analyses of who is in jail or prison for marijuana found that less than 0.7% of all state inmates were behind bars for marijuana possession only (with many of them pleading down from more serious crimes).[1] Other independent research has shown that the risk of arrest for each “joint,” or cannabis cigarette, smoked is about 1 arrest for every 12,000 joints.[2] This probably explains the fact that the literature on early decriminalization effects on use has been mixed. Some studies found no increase in use in the so-called “depenalization” states, whereas others found a positive relationship between greater use and formal changes in the law.[3]
The more recent discussion about state-level legalization may provide more insights. Two RAND Corporation reports concluded that legalization would result in lower cannabis prices, and thus increases in use (though by how much is highly uncertain), and that “legalizing cannabis in California would not dramatically reduce the drug revenues collected by Mexican drug trafficking organizations from sales to the United States.”[4]
5. Marijuana advocates don't like to hear it, but pot is addictive for some users. Where do you stand on this controversial issue?
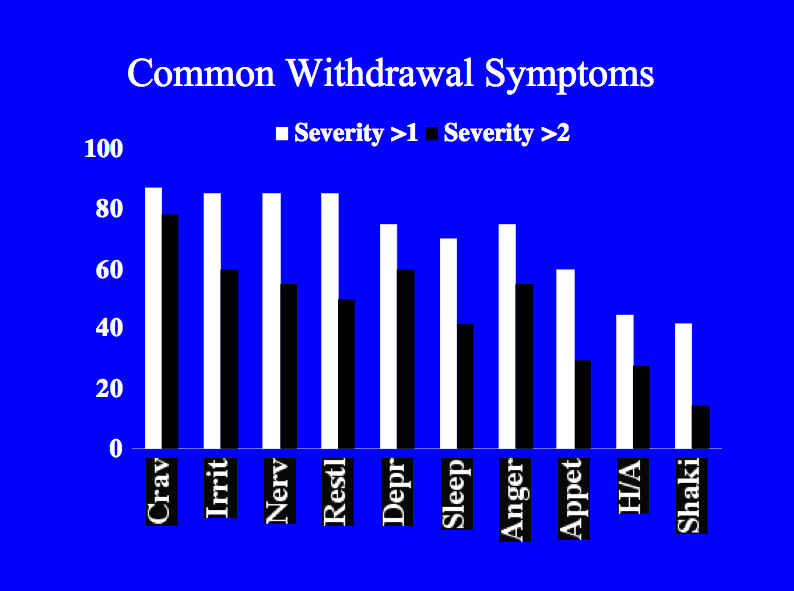
Science tells us that marijuana is addictive—about 1 in 11 people who ever smoke marijuana are addicted; but if you start in adolescence that number climbs to 1 in 6. That's not anyone's opinion but rather the result of rigorous scientific research done by the National Institutes of Health and confirmed by other international scientific bodies. Is marijuana as addictive as tobacco cigarettes? No. The addiction rate for tobacco is about 1 in 3; for heroin it is lower, about 1 in 4. Users who try to quit experience withdrawal symptoms that include irritability, anxiety, insomnia, appetite disturbance, and depression.
A United States study that dissected the National Longitudinal Alcohol Epidemiologic Survey (conducted from 1991 to 1992 with 42,862 participants) and the National Epidemiologic Survey on Alcohol and Related Conditions (conducted from 2001 through 2002 with more than 43,000 participants) found that the number of cannabis users stayed the same while the number dependent on the drug rose 20 percent from 2.2 million to 3 million.[5]Authors speculated that higher potency marijuana may have been to blame for this increase. As I've heard said many times by experienced tokers, "this isn't your Grandfather's Woodstock Weed."
[1] “Substance Abuse and Treatment, State and Federal Prisoners, 1997.” BJS Special Report, January 1999, NCJ 172871. http://www.ojp.usdoj.gov/bjs/pub/pdf/satsfp97.pdf
[2] Beau Kilmer, Jonathan P. Caulkins, Rosalie Liccardo Pacula, Robert J. MacCoun, Peter H. Reuter, Altered State? Assessing How Cannabis Legalization in California Could Influence Cannabis Consumption and Public Budgets, RAND, 2010.
[3] For a discussion see MacCoun, R., Pacula, R. L., Reuter, P., Chriqui, J., Harris, K. (2009). Do citizens know whether they live in a decriminalization state? State cannabis laws and perceptions. Review of Law & Economics, 5(1), 347-371.
[4] Beau Kilmer, Jonathan P. Caulkins, Rosalie Liccardo Pacula, Robert J. MacCoun, Peter H. Reuter, Altered State? Assessing How Cannabis Legalization in California Could Influence Cannabis Consumption and Public Budgets, RAND, 2010. And see Kilmer, Beau , Jonathan P. Caulkins, Brittany M. Bond and Peter H. Reuter. Reducing Drug Trafficking Revenues and Violence in Mexico: Would Legalizing Cannabis in California Help?.Santa Monica, CA: RAND Corporation, 2010. http://www.rand.org/pubs/occasional_papers/OP325. Also available in print form.
[5] ]Compton, W., Grant, B., Colliver, J., Glantz, M., Stinson, F. Prevalence of Cannabis Use Disorders in the United States: 1991-1992 and 2001-2002Journal of the American Medical Association.. 291:2114-2121.














{kind=link}
{kind=link}