Federal study also discusses medical marijuana.

Considering the impasse on marijuana policy between state and federal governments in the U.S., the primary government agency in charge of drug research—NIDA, the National Institute on Drug Abuse—would seem to be caught between a rock and a hard place. Neuroscientists and other marijuana investigators who do research under NIDA grants have a fine line to walk in their efforts to disseminate research findings on cannabis.
From a public health point of view, NIDA is expected to keep up the pressure against drug legalization, or at least keep out of the fight, while also researching the medical pros and cons of cannabis. So it was with some interest that drug policy officials took in a recent article in the New England Journal of Medicine by NIDA director Nora Volkow titled “Adverse Health Effects of Marijuana Use.”
While the press has understandably centered on the risk of marijuana use among teens, which is the focus of the study, the report also contains some surprising admissions about marijuana’s health benefits as well as its addictive potential.
The teen risk emphasis comes from recent studies on two fronts—impaired driving and impaired brain function. The first is seriously confounded by dual use with alcohol, and the second is based, at least in part, on a controversial long-term study showing that marijuana use in the early years demonstrably lowers adult IQs.
No one would suggest that heavy marijuana smoking is good for developing teen brains, and there is sufficient evidence to worry about impairment to memory and to certain so-called “executive” cognitive functions. It is not clear how lasting these effects can be, but lead author Volkow is confident enough to say in a prepared statement that “Physicians in particular can play a role in conveying to families that early marijuana use can interfere with crucial social and developmental milestones and can impair cognitive development.”
That these negative effects can be the outcome of heavy pot smoking in the teen years seems established beyond reasonable doubt. The extent and duration of these negative outcomes remain the topic of vociferous debate—although it is increasingly clear that the body’s endogenous cannabinoid system plays a key role in synapse formation during early brain development.
Meanwhile, the report re-emphasized the fact that marijuana is an addictive drug for some users—a fact that should not need re-emphasizing, but, lamentably, does. As Volkow and her co-authors write: “The evidence clearly indicates that long-term marijuana use can lead to addiction. Indeed, approximately 9% of those who experiment with marijuana will become addicted.”
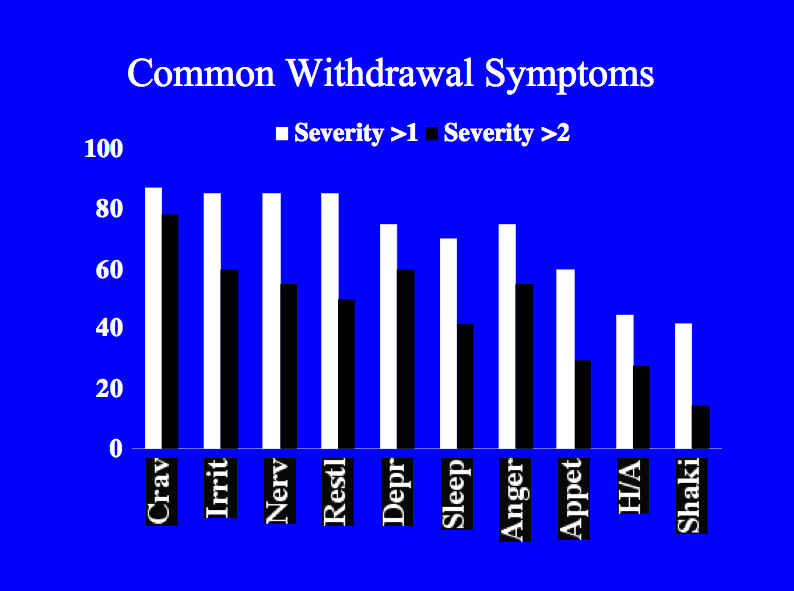
Moreover, as regular readers of Addiction Inbox already know, “there is also recognition of a bona fide cannabis withdrawal syndrome (with symptoms that include irritability, sleeping difficulties, dysphoria, craving, and anxiety), which makes cessation difficult and contributes to relapse.” And, in line with the report’s overall theme, “those who begin in adolescence are approximately 2 to 4 times as likely to have symptoms of cannabis dependence within 2 years after first use.”
To their credit, the investigators decline to endorse the claim that marijuana use exacerbates or initiates episodes of illness in patients with schizophrenia and other psychoses, noting that “it is inherently difficult to establish causality in these types of studies because factors other than marijuana use may be directly associated with the risk of mental illness.” Furthermore, while early marijuana use is associated with an increased risk of dropping out of school, “reports of shared environmental factors that influence the risks of using cannabis at a young age and dropping out of school suggest that the relationship may be more complex…. The relationship between cannabis use by young people and psychosocial harm is likely to be multifaceted, which may explain the inconsistencies among studies.”
Indeed. The report also declares that the effects of long-term pot smoking on the risk of lung cancer are “unclear,” and that “the smoking of cigarettes containing both marijuana and tobacco products is a potential confounding factor with a prevalence that varies dramatically among countries.”
In conclusion, the strict demands of causality mean that the long-term effect of chronic marijuana exposure is not known with any certainty. It is possible, even likely, that these effects can vary dramatically from one smoker to another. But the equally persuasive demands of common sense dictate that inhaling dried, super-heated vegetable matter on a regular basis is likely to degrade your health, the more so if you are young and healthy to begin with.
As for other health issues: “The authoritative report by the Institute of Medicine, Marijuana and Medicine, acknowledges the potential benefits of smoking marijuana in stimulating appetite, particularly in patients with the acquired immunodeficiency syndrome (AIDS) and the related wasting syndrome, and in combating chemotherapy-induced nausea and vomiting, severe pain, and some forms of spasticity. The report also indicates that there is some evidence for the benefit of using marijuana to decrease intraocular pressure in the treatment of glaucoma.”
A detailed section titled “Clinical Conditions with Symptoms That May Be Relieved by Treatment with Marijuana or other Cannabinoids” brought additional research to light:
—Glaucoma: “More research is needed to establish whether molecules that modulate the endocannabinoid system may not only reduce intraocular pressure but also provide a neuroprotective benefit in patients with glaucoma.”
—Nausea: “THC is an effective antiemetic agent in patients undergoing chemotherapy, but patients often state that marijuana is more effective in suppressing nausea…. Paradoxically, increased vomiting (hyperemesis) has been reported with repeated marijuana use. [See various blog posts by Drugmonkey and me, starting with this and this.]
—AIDS-associated conditions: “Smoked or ingested cannabis improves appetite and leads to weight gain and improved mood and quality of life among patients with AIDS.”
—Chronic pain: “Studies have shown that cannabinoids acting through central CB1 receptors, and possibly peripheral CB1 and CB2 receptors, play important roles in… various models of pain. These findings are consistent with reports that marijuana may be effective in ameliorating neuropathic pain, even at very low levels of THC.”
—Inflammation: “Cannabinoids (e.g., THC and cannabidiol) have substantial anti-inflammatory effects…. Animal models have shown that cannabidiol is a promising candidate for the treatment of rheumatoid arthritis and for inflammatory diseases of the gastrointestinal tract (e.g., ulcerative colitis and Crohn’s disease).”
—Multiple sclerosis: “Nabiximols (Sativex, GW Pharmaceuticals), an oromucosal spray that delivers a mix of THC and cannabidiol, appears to be an effective treatment for neuropathic pain, disturbed sleep, and spasticity in patients with multiple sclerosis. Sativex… is currently being reviewed in phase 3 trials in the United States in order to gain approval from the Food and Drug Administration.”
—Epilepsy: In a recent small survey of parents who use marijuana with a high cannabidiol content to treat epileptic seizures in their children, 11% reported completed freedom from seizures…. Although such reports are promising, insufficient safety and efficacy data are available on the use of cannabis botanical for the treatment of epilepsy. However, there is increasing evidence of the role of cannabidiol as an antiepileptic agent in animal models.”
Volkow N.D., Baler R.D., Compton W.M. & Weiss S.R.B. Adverse health effects of marijuana use., The New England journal of medicine, PMID: 24897085




 nicotine
nicotine
